Life with
CEREBRAL PALSY
Cerebral palsy (CP) is a common physical disability that is diagnosed during childhood. It is a group of neurological permanent disorders that are non-progressive.
Cerebral Palsy was first described in 1862 by the orthopaedic surgeon William Little. Today, the International Executive Committee defines cerebral palsy as:
The overall prevalence of CP is 2.11 per 1000 live births (95% CI 1.98–2.25) 2
The prevalence is highest in children weighing 1000 to 1499g at birth (59.18 per 1000 live births; 95% CI 43.38–73.95), and lowest in children weighing over 2500g at birth (1.33 per 1000 live births; 95% CI 1.19–1.49).2
As a result, interventions, such as electronic foetal monitoring and caesarean section, increased with time.3
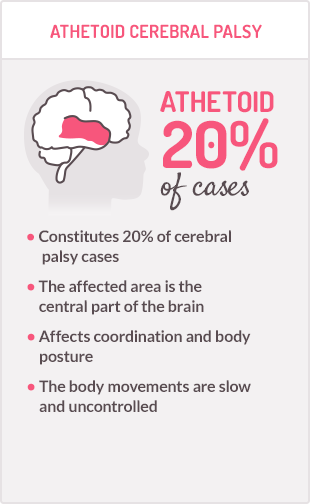
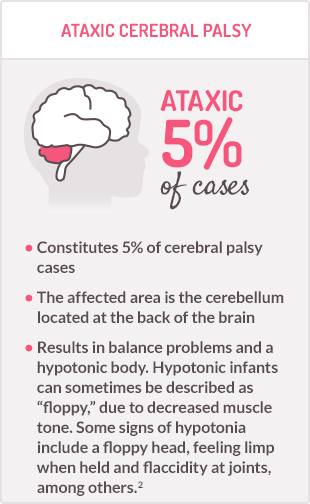
There are many different types of CP, which vary in the parts of the body that are affected, the type of impairment and the severity of mobility limitations.
→Click to learn about the different types of CP
CP has a major impact on the child’s and caregiver’s quality of life.4 Caregivers are under a lot of pressure, and implications can affect their overall quality of life. With your help, caregivers and patients can overcome such challenges and improve their daily life. A better understanding of the emotional journey that caregivers go through may help you in finding solutions and/or recommendations to empower them.
References:
- Colver A et al. Cerebral palsy. Lancet. 2014;383:1240-49.
- Oskoui M et al. An update on the prevalence of cerebral palsy: a systematic review and meta-analysis. Dev Med Child Neurol. 2013;55(6):509-19.
- Reddihough DS and Collins KJ. The epidemiology and causes of cerebral palsy. Aust J Physiother. 2003;49(1):7-12.
- Eunson P. Aetiology and epidemiology of cerebral palsy. Symposium: Cerebral Palsy. Paediatrics and Child Health.2016;26:9:367-372.
Cerebral palsy (CP) can be diagnosed several months after birth, or even years later. Usually, CP is diagnosed before the age of three.
The diagnosis is essentially clinical. A systematic approach, focusing on maternal, obstetric and perinatal histories, a review of developmental milestones and a thorough neurological examination and observation of the child in various positions (supine, prone, sitting, standing, walking and running) is mandatory.
The symptoms are complex and vary depending on the types and degrees of motor impairment. You can read all about the degree of motor impairment in the following section
→Click to learn about the different types of CP
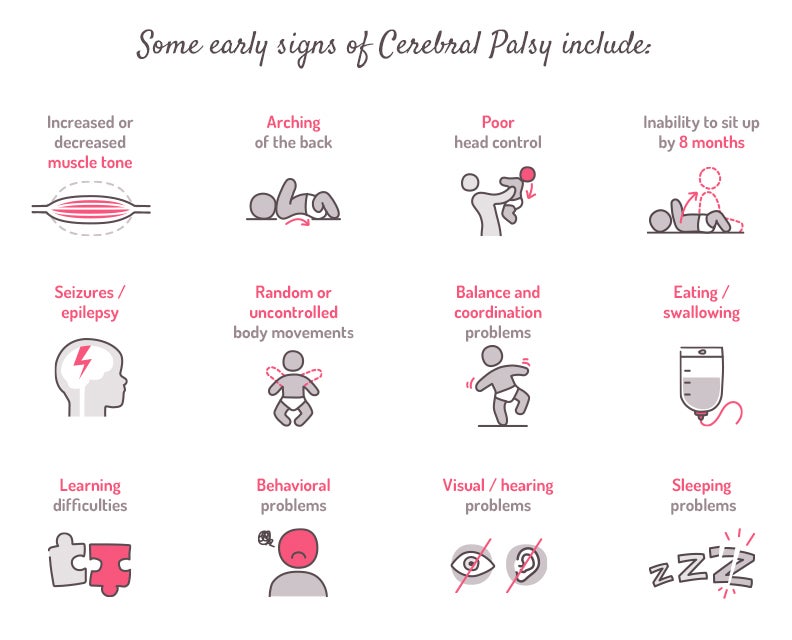
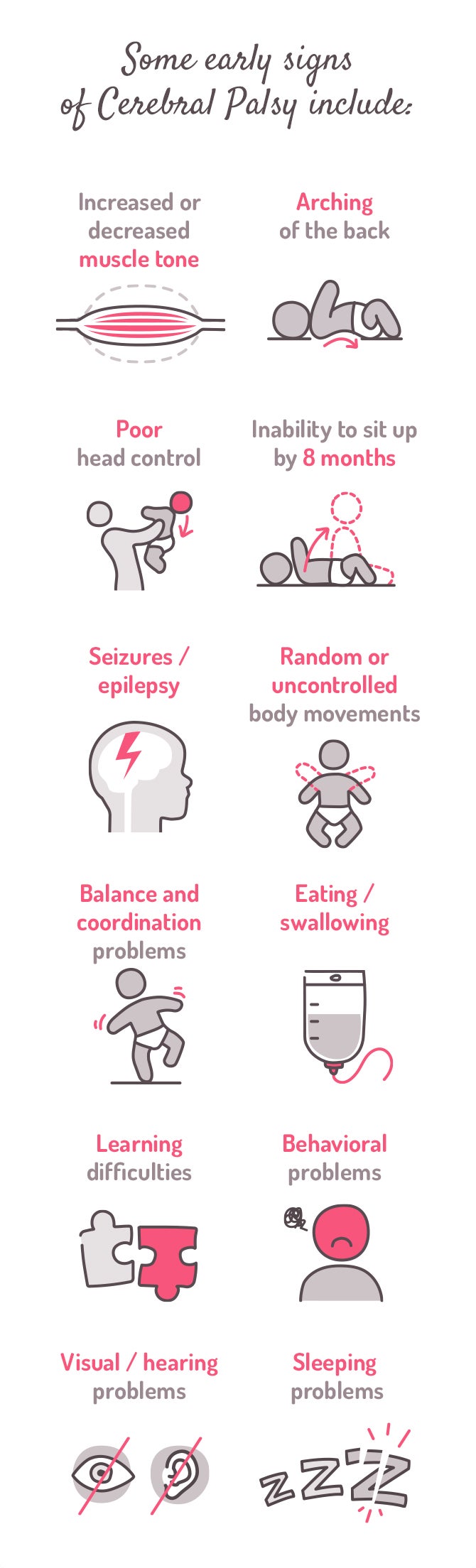
Some early signs of CP may include:1,2
Unfortunately, children with CP will most probably have multiple disabilities. 80% will have at least one associated disability, while 40% will have three or more.3
References:
- Colver A et al. Cerebral palsy. Lancet. 2014;383:1240-49.
- National Institute for Health and Care Excellence. Cerebral palsy in under 25s: assessment and management. Full Guideline. NG62. 2017. Available at:https://www.nice.org.uk/guidance/ng62/evidence/full-guideline-pdf-4357166226
- Cerebral Palsy. Critical elements of Care. Center of Children with Special Needs, Seattle Children’s Hospital. Seattle. WA, Fifth Edition. 2011; 4-9
Each child with cerebral palsy (CP) is unique, with varying abilities and disabilities. Nonetheless, severity can be generally classified according to the type of motor function impairment and the part of the body that is mostly affected.
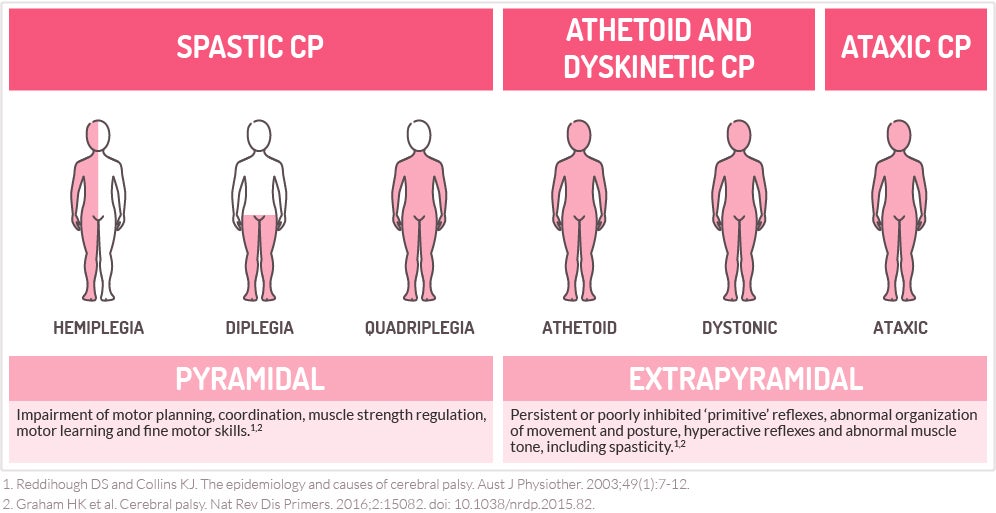
Quadriplegia affects all 4 limbs (arms and legs), diplegia affects 2 limbs (typically both legs) and hemiplegia, or unilateral CP affects one arm and one leg on the same side of the body1.
The types of CP include:2,3,4,5,6
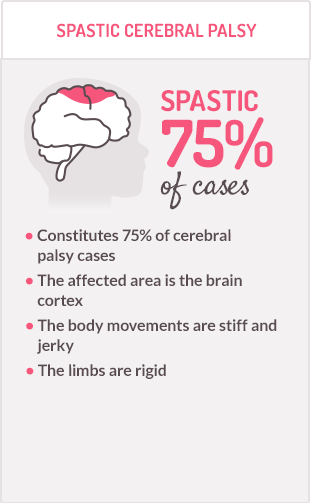
Motor symptoms of cerebral palsy can be divided depending on the location of the lesion and which motor tracts are affected (pyramidal or extrapyramidal).
The following illustration shows the motor syndromes associated with different types of CP.8
Motor syndromes of cerebral palsy
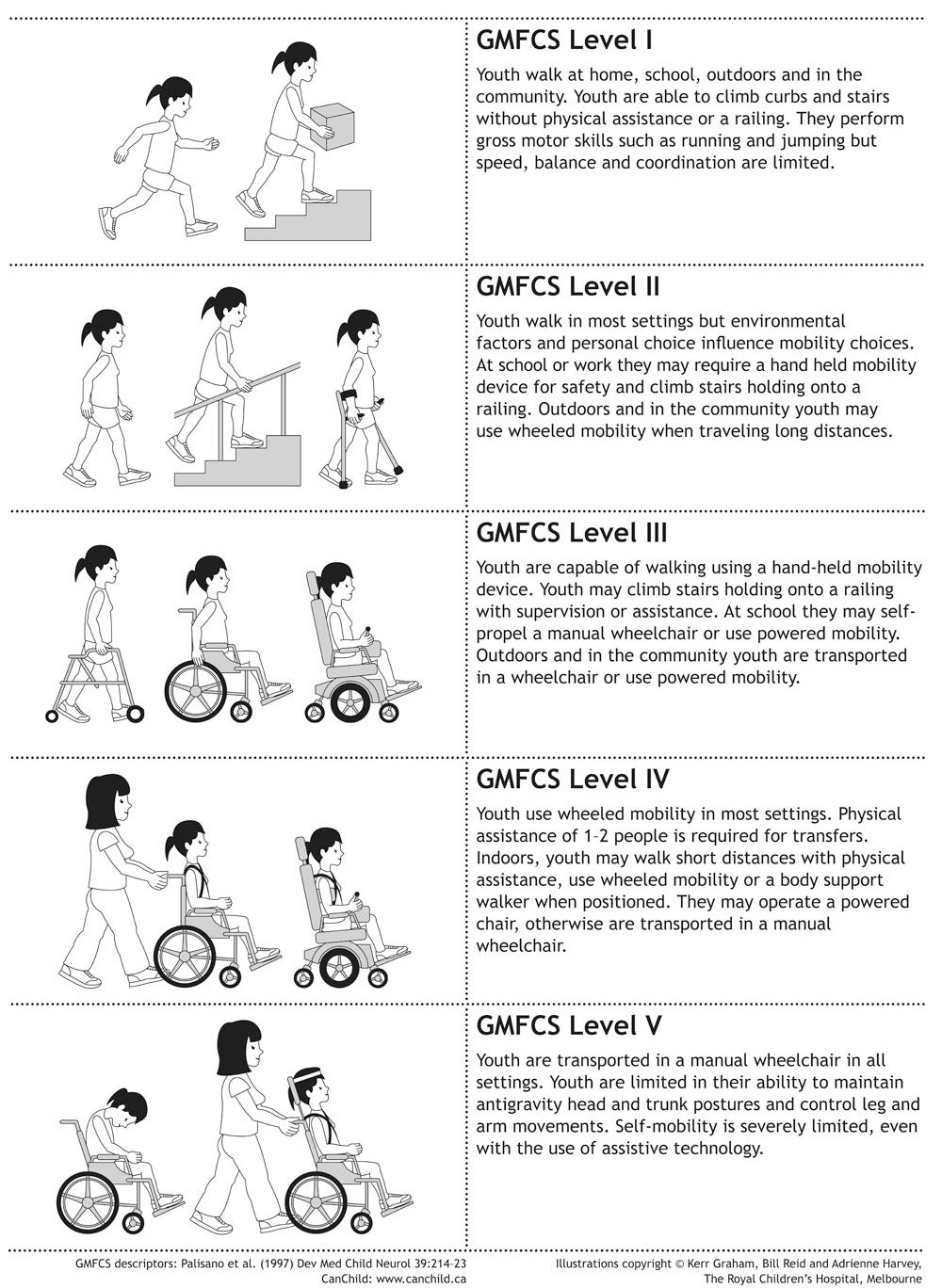
The severity of CP mobility limitations can also be categorized into 5 different levels, according to the Gross Motor Function Classification System (GMFCS).9 Each level clearly describes the child’s current physical abilities and whether equipment or mobility aids are or will be needed in the future.
GMFCS E & R between 6th and 12th birthday: Descriptors and illustrations

GMFCS E & R between 12th and 18th birthday: Descriptors and illustrations





It is important to recognize the diversity in CP cases and that every child with CP is unique, requiring personalised, tailored care.
References:
- Reddihough DS and Collins KJ. The epidemiology and causes of cerebral palsy. Aust J Physiother. 2003;49(1):7-12.
- Odding E,Disabil Rehabil 2006 28;28(4):183-91.
- Dahlseng MO,Dev Med Child Neurol 2012;54(10):938-44.
- Carnahan KD,BMC Musculoskeletal Disorders 2007;8:50.
- Andersen GL,Eur J Paediatr Neurol 2008;12(1):4-13.
- Sigurdardóttir S, Dev Med Child Neurol 2009;51:356–363.
- Prasad AN and Prasad C. Genetic evaluation of the floppy infant. Semin Fetal Neonatal Med. 2011;(16):99-108.
- Graham HK et al. Cerebral Palsy. Nat Rev Dis Primers. 2016;2:15082. doi: 10.1038/nrdp.2015.82
- Palisano R et al. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol. 1997;39(4):214-23.